Contents
Summary Background Purpose of Retreat Retreat Outcomes Focus Area Discussion Overviews I. Financing and Policy Changes Problem Statement and Background Key Ideas and Proposals II. Country Transitions Problem Statement and Background Key Ideas and Proposals III. Commodities Problem Statement and Background Key Ideas and ProposalsThis document represents a summary of discussions from a family planning leadership retreat co-convened by the Center for Global Development and the Kaiser Family Foundation on January 18-19, 2018, in Washington, DC. While it reflects the main ideas of the retreat participants, it is not a consensus document and is not intended to represent the views of any individual or organization. This document was prepared by Felice Apter, Amanda Glassman, and Janeen Madan Keller (Center for Global Development) and Jen Kates, Kellie Moss, and Adam Wexler (Kaiser Family Foundation). Jessie Lu assisted with overall development and production. The authors are grateful for contributions from the Bill & Melinda Gates Foundation in support of this work.
Summary
Background
The international family planning community has made impressive gains in increasing global access to high-quality, voluntary family planning services. As of July 2017, 309 million women and girls in 69 FP2020 countries were using a modern method of contraception, representing an increase of 38.8 million users since 2012.[1] However, significant challenges remain with maintaining current support and meeting the growing need projected for family planning services and commodities across low- and middle-income countries (LMICs). A key challenge is the uncertainty surrounding future funding for such efforts from international donors in particular, but also from host country budgets. These concerns are further exacerbated by the political landscape in the United States—the largest single donor to global family planning efforts—including proposals to significantly cut the US international family planning budget as well as other policy changes. Given the current climate, a forward-looking agenda to address the potential implications of increasing unpredictability in future funding as well as policy shifts for family planning programs is more important than ever.
Purpose of Retreat
Through their respective analytic work tracking funding and policy trends in family planning and linking those changes to larger global health and development paradigms, the Center for Global Development (CGD) and Kaiser Family Foundation (KFF) identified a need to discuss the implications of uncertainty in the global family planning landscape for policy, programs, and people. To this end, CGD and KFF convened a family planning leadership retreat on January 18-19, 2018, that brought together a range of stakeholders from the international family planning space, as well as the broader global health and development community. Participants included US government officials, other donors and international organizations, NGOs, and the private sector.
The meeting was designed to identify practical strategies and approaches going forward. Three interconnected focus areas were identified as high priority:
- Financing and Policy Changes: Uncertainty of future donor support and financing implications of policy changes;
- Country Transitions: Acceleration of country transition timelines and realistic assessment of domestic resource mobilization opportunities; and
- Commodities: Possible decreases in support for commodities and country supply chains.
The retreat included overview presentations in each of these three focus areas followed by related break-out sessions to more specifically identify strategies for further consideration.
Retreat Outcomes
The retreat’s discussions yielded several cross-cutting themes across the three focus areas: 1) improve donor alignment; 2) measure and mobilize domestic resources; 3) fill data gaps; 4) support integration while maintaining a focus on family planning; and 5) recognize that uncertainty also provides opportunity. These are discussed in more depth below. In addition, concrete ideas for potential approaches and strategies in each of the three focus areas are provided in Table 1 and in individual discussion overviews.
- IMPROVE DONOR ALIGNMENT: The need for enhanced donor alignment of family planning investments is not new, but it has taken on increased urgency in the current environment.[2] In particular, participants identified improved alignment around country selection and prioritization for funding, with a focus on which countries or sub-regions might be most vulnerable to short-term funding reductions, as an urgent need. Coordination around longer-term planning as countries transition from aid eligibility is also needed. Participants also discussed the need to examine and reduce donor inefficiencies at the country and global levels (e.g., addressing parallel supply chains). Short-term strategies can be designed with the goal of serving as a bridge to longer-term strategies for sustainable funding and program self-sustainability.
- MEASURE AND MOBILIZE DOMESTIC RESOURCES: Participants identified a critical need to better understand the landscape of domestic resources for family planning, including current spending levels by national governments, fiscal space for additional spending, and political will. Such assessments should be pragmatic and will need to consider the difficulties in tracking family planning-specific expenditures within national budgets and challenges around accounting transparency more generally. It is also important to be cognizant of the fact that countries may be experiencing multiple aid transitions in areas beyond family planning, as well as other overarching development challenges, magnifying budget pressures. Furthermore, considerations of fiscal space for family planning should recognize that national governments have competing priorities both within and outside the health sector. Understanding each country’s fiscal space and political will can help donors program resources most effectively. In addition, building capacity in such areas as contracting, developing insurance schemes, and financial tracking will be an important component of efforts to ensure greater government self-sufficiency.
-
FILL DATA GAPS: Participants identified several areas where critical data gaps limit the ability of policymakers, implementers, and other stakeholders to plan effectively. These include the lack of data on:
- Relative effectiveness of key investments
- Overall projected cost to meet family planning need across both the public and private sectors
- Improved understanding of family planning service costs
- Current domestic expenditures for family planning[3]
- Measures of fiscal space
Working to fill these data gaps will be important for informing planning and decision-making going forward.
- SUPPORT INTEGRATION WHILE MAINTAINING A FOCUS ON FAMILY PLANNING: The importance of integrating family planning with other global health and development programs, where possible, was highlighted. Indeed, for the past several years, PEPFAR has sought to increase integration of family planning and HIV programs, and currently, USAID is seeking greater integration across global health programs. At the same time, participants discussed the need to ensure that family planning efforts do not get diluted or minimized through integration, particularly given the often-politicized nature of debates about US family planning efforts.
- RECOGNIZE THAT UNCERTAINTY ALSO PROVIDES OPPORTUNITY: Although discussions focused largely on the challenges that accompany donor uncertainty, participants identified several important opportunities. There was emphasis on transition as an opportunity to better understand countries’ progress and needs and to strengthen implementation of, and achieve efficiencies in, international family planning assistance. Moreover, increased downward pressure on budgets also presents an opportunity to better harmonize investments across donors and channel available resources to areas of greatest need.
TABLE 1: KEY IDEAS AND PROPOSALS BY FOCUS AREA
| I. Financing and Policy Changes |
|---|
|
| II. Country Transitions |
|
| III. Commodities |
|
Focus Area Discussion Overviews
I. Financing and Policy Changes
Problem Statement and Background
Donor government funding for family planning is on the decline and future funding from the single largest donor—the United States—is uncertain. In addition, a number of recent US policy decisions regarding family planning contribute to this uncertainty.
Figure I-A
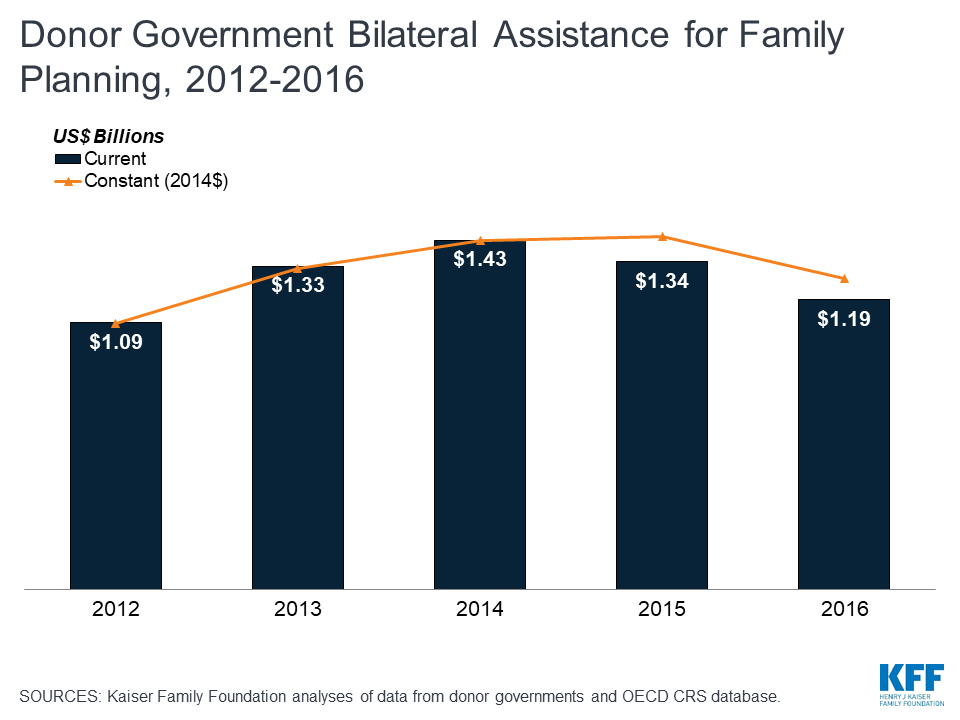
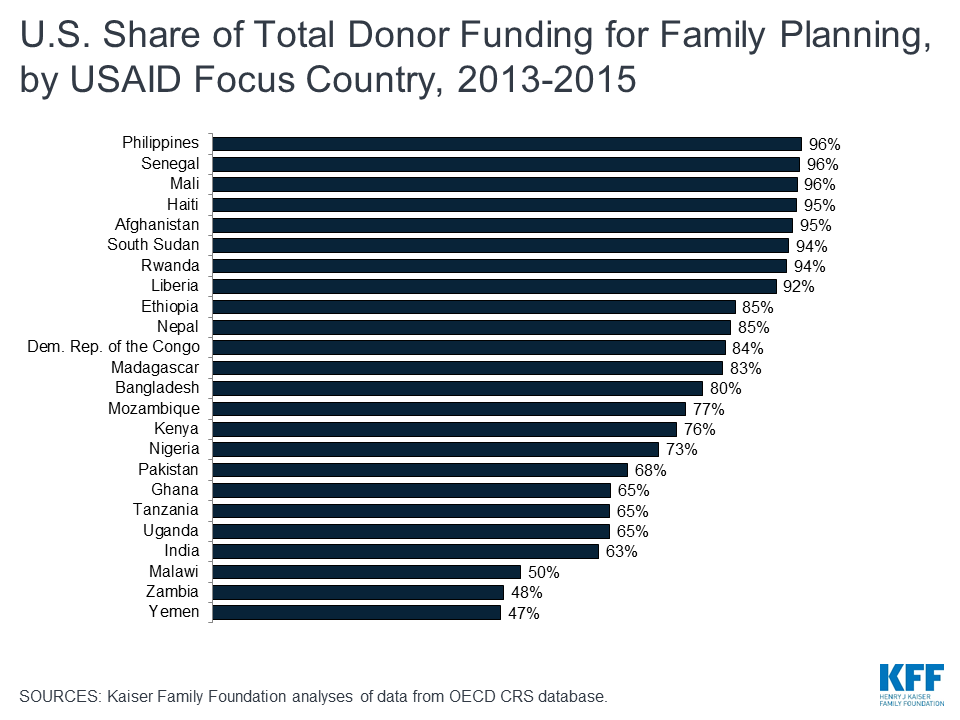
Recent analysis finds that donor government funding for family planning is on the decline, even after accounting for currency fluctuations and other factors (see Figure I-A).[4] Moreover, future funding is uncertain in large part due to the current fiscal and policy environment in the United States, the single largest government donor to family planning (providing 45 percent of bilateral funding in 2016). The Trump administration has proposed deep budget cuts to global family planning, including zeroing out the global family planning program budget in the President’s FY 2018 budget request. Congress has indicated that it will not support cuts of this magnitude, as evidenced by the FY 2018 Omnibus that included $607.5 million for family planning/reproductive health, matching the FY 2017 enacted level.[5] However, the administration’s proposals to significantly reduce global family planning funding continue.[6] Furthermore, the larger backdrop of US budgetary challenges is putting downward pressure on discretionary spending across the board. Because the US is the largest government donor to family planning, partner countries are particularly vulnerable to any potential US cuts. This is even more pronounced in the 24 USAID family planning priority countries,[7] where the US provides an estimated 76 percent of donor support overall, including more than 90 percent in eight of these countries (see Figure I-B).[8]
In addition, a number of recent US policy decisions regarding family planning further contribute to uncertainty. These include the administration’s withholding of funding to the United Nations Population Fund (UNFPA) under the Kemp-Kasten Amendment[9] and the reinstatement and expansion of the Mexico City Policy (MCP), renamed Protecting Life in Global Health Assistance (PLGHA)[10] by the current administration. On the latter, there remain many unanswered questions about the policy’s impact, but early analyses indicate that the expanded policy could apply to more than $7 billion in global health funding and, by conservative estimates, more than 1,000 foreign NGOs, likely leading to service coverage gaps in some geographic areas and for some populations.[11]
Figure I-B
Key Ideas and Proposals
Overarching Discussion Goal: Given uncertainty surrounding future family planning funding, it will be important for the main financing actors to engage in a more structured, transparent, and harmonized contingency planning process to help drive a rational prioritization of resources.
Participants identified ways to address and potentially mitigate financial and policy uncertainty, including:
-
SUPPORT A MORE SYSTEMATIC ASSESSMENT OF COUNTRY VULNERABILITIES TO CHANGES IN EXTERNAL FINANCING, INCLUDING IDENTIFYING FACTORS/INDICATORS THAT COULD BE USED TO HELP PREDICT VULNERABILITY.
-
Participants discussed the need for clear and consistent metrics to assess the vulnerability of countries to changes in financing, including identifying metrics for measuring vulnerability.
- Among the factors discussed were country income classification; other financial resources available (external and domestic sources); social insurance; and vulnerability of populations (including adolescents, women, and girls in humanitarian contexts).
- Donors take varying approaches to country prioritization, using different criteria and processes. A review of their respective prioritization methodologies could allow donors, including USAID, and other stakeholders to proactively identify countries with the most need of external assistance and to scale funding flows accordingly.
- There was discussion on how funding uncertainty affected USAID country mission decisions, which, in turn, could make some countries more vulnerable to changes. Specifically, it was noted that, faced with uncertainty, some missions may choose not to include family planning in their future country strategy and budget requests, which could affect actual services in the field.
- Lastly, participants felt it was important to not just focus on country and implementer vulnerability; rather, it was also important to understand and document factors supporting resilience. Identification and documentation of lessons learned from countries, implementers, platforms, etc., that have demonstrated resilience to financial and policy changes and uncertainties could provide insight to future decision-making.
-
Participants discussed the need for clear and consistent metrics to assess the vulnerability of countries to changes in financing, including identifying metrics for measuring vulnerability.
-
RE-EXAMINE THE METHODOLOGY USED FOR PRIORITIZING USAID FAMILY PLANNING COUNTRIES TO SET THE STAGE FOR ENHANCED DONOR COORDINATION.
- Participants discussed how best to prioritize US family planning priority countries/investments, the challenges to doing so, and opportunities for doing it better.
- While USAID supports family planning programs in approximately 40 countries, it focuses its effort in 24 high-priority countries and the Ouagadougou Partnership countries. Such prioritization can serve many purposes, including helping to focus limited resources where need is greatest; assisting with contingency planning given funding uncertainty; and allowing for more proactive transition planning as the United States Government (USG) seeks to decrease its investments and in turn increase host country government spending over time. In the case of USAID’s family planning program, these 24 countries also align with US maternal and child health (MCH) investments (23 of the 24 countries are also USAID MCH priority countries).
- At the same time, the list of priority countries has been static for many years,[12] raising questions about whether there are better ways to prioritize countries to address emerging gaps or other challenges (e.g., the use of S-curves depicting the growth trajectory of modern contraceptive prevalence[13]).
- In addition to prioritizing countries, participants discussed the need to better assess prioritization of service delivery within countries across both public and private sectors. Such efforts could be significantly aided with better data on service effectiveness. Key questions to ask might include: What is the most impactful set of services to support in a particular country? How could greater efficiencies be achieved? Are there interventions that should no longer be invested in? Can interventions be better matched programmatically and geographically to their positions on the modern contraceptive prevalence rate S-curve? Participants also asked what lessons could be learned from PEPFAR, which has undertaken such an exercise across their activities and redirected investments to more effective services.
- Another issue raised was the need to map the range of donor family planning investments and country prioritization approaches. This not only could help to “right size” investments or redirect investments to where they are needed most, but also help to assess country vulnerabilities to funding shifts. For instance, donors might find instructive analyses of data like that in Figure I-B, which shows US family planning investments as a share of all donor investments in the 24 USAID family planning priority countries. Such analyses could be expanded to include all FP2020 countries.[14]
- Finally, it will be important for any family planning prioritization effort to be connected to USAID’s larger, agency-wide effort to harmonize country prioritization across programs and to identify factors that support country self-sufficiency.[15]
-
IDENTIFY WAYS IN WHICH THE LARGER FAMILY PLANNING COMMUNITY CAN SUPPORT A USG COUNTRY PRIORITIZATION PROCESS AND VULNERABILITY ASSESSMENT IN THE CONTEXT OF FUNDING UNCERTAINTY.
-
Participants identified several key areas where the larger community could support this process, including:
- Proactively identifying the changes that could occur;
- Convening leadership across donors to develop a plan to minimize disruption of family planning commodities and services in both public and private sectors;
- Identifying the capacity of other stakeholders to step in, including prioritizing support to any gaps created by the loss of US technical leadership; and
- Developing a strategy to measure and track the impact of “shocks” (e.g., funding reductions, abrupt transitions, policy changes) in 1) outcomes, 2) processes, 3) shifts in implementers and providers (including costs associated with these changes), and 4) lessons.
-
Participants identified several key areas where the larger community could support this process, including:
-
WITH THE REINSTATEMENT AND EXPANSION OF MCP/PLGHA, THE USG AND/OR OTHER STAKEHOLDERS COULD DEVELOP A PROCESS TO IDENTIFY WHERE GAPS IN FAMILY PLANNING ACCESS ARE MOST LIKELY TO OCCUR AND, WHERE GAPS EXIST, IDENTIFY OTHER SOURCES OF FUNDING AND/OR ALTERNATE IMPLEMENTERS.
- Participants stated that short-term efforts are needed to identify anticipated gaps and alternate sources of funding and implementers.
-
Participants discussed the many kinds of impact assessments that are needed to build on the USG efforts (some of which are underway) including:
- short-term, more “real-time” assessments to identify needs and gaps; and
- longer-term research (since the time between congressional appropriation and USAID programming means that effects of decreased funding and policy change may not be felt for several years).
- The types of impacts to predict and assess include immediate service gaps, adverse health outcomes, effects on sustainability, and the additional costs of having to respond to the policy and/or seek new implementers.
- As gaps or needs are identified, the community coordination effort should include more recent initiatives and newly engaged donors—SheDecides is one possible mechanism.[16]
-
THE MAIN FAMILY PLANNING FINANCING ACTORS (BILATERAL DONORS, GLOBAL FINANCING FACILITY, UNFPA, WORLD BANK, PRIVATE DONORS, THE PRIVATE SECTOR) COULD MORE PROACTIVELY ENGAGE IN ASSESSING AND RESPONDING TO FAMILY PLANNING AID VULNERABILITIES AND PRIORITIZING ALLOCATIONS USING EXISTING FORA.
- It was noted that existing venues that bring together the main family planning stakeholders could be utilized more proactively and purposefully to discuss prioritization and planning for such change or “shocks” (e.g., funding reductions, abrupt transitions, policy changes). Specifically, participants identified the FP2020 Initiative as a potential vehicle for such efforts, including its Reference Group and Country Technical Teams.[17]
- These existing mechanisms are well poised to facilitate such discussions, which could be expanded to include other stakeholders (e.g., SheDecides) that may have resources to contribute.
-
ENHANCE EFFORTS TO TRACK DOMESTIC RESOURCES FOR FAMILY PLANNING, INCLUDING ASSESSMENTS OF FISCAL SPACE AND POLITICAL WILL NEEDED TO SUPPORT INCREASED DOMESTIC INVESTMENT.
- While there is a global estimate of the share of family planning expenditures provided by domestic governments (29 percent), data on domestic expenditures is significantly limited at this time.[18] This was identified by participants as a critical data need. While there is work underway to assess what is currently being spent, it is limited to a subset of countries and will take some time.[19]
-
Key points raised included the following:
- It will be important to work with national governments to assist with resource tracking efforts, including through technical assistance. In some cases, systems may not be in place to easily track expenditures by program area; family planning may not be programmed as a separate line item; and/or some countries are decentralizing health programming and funding.
- Experience suggests there is fiscal space for governments to increase their investments in family planning, but political will is also needed if such investments are to be secured; assessing political will, therefore, also be critical.[20]
- The US and other donors can work with countries to enhance the incentives to increase resources from their governments and to support/maintain the political will to do so; in some cases, this may also include the need to address increasingly decentralized decision-making.
-
To the extent that the US and other donors decide to transition out of countries, it will be important to provide technical assistance to support successful transitions, even when domestic resources are available.
- Areas identified include supporting countries and local NGOs in developing ways to strengthen contracting mechanisms, including addressing payment delays from governments to NGOs; regarding the latter, some suggested that the USG or other donors could serve as a guarantor of government payments to support implementers of service delivery.
-
UTILIZE INNOVATIVE FINANCING INSTRUMENTS, WHERE APPROPRIATE, TO INCENTIVIZE SUSTAINABILITY.
-
Discussions covered several possible approaches (note: while these approaches could relate to family planning programs more broadly, they could also take a more specific focus on commodities, for example).
- Interest-free loans (e.g., DfID – 50 years, no interest);
- Bridge funding mechanisms (e.g., UNICEF Vaccine Independence Initiative[21]), revolving funds (e.g., PAHO Revolving Fund[22]);
- Joint trust funds to secure longer-term investments (e.g., International Finance Facility for Immunization[23]);
- Debt relief / debt buy-downs (either for family planning alone and/or the larger health portfolio as long as commodities are included); and
- Banks or donors serving as guarantors (note: there was some concern about fees charged by for-profit entities).
-
Discussions covered several possible approaches (note: while these approaches could relate to family planning programs more broadly, they could also take a more specific focus on commodities, for example).
II. Country Transitions
Problem Statement and Background
Family planning gains may be at risk due to possible abrupt and/or accelerated country transitions by donors, including the US. At the same time, there is an opportunity to carefully plan and execute strategic transitions in close partnership with countries, which could in turn help to alleviate pressure on tight donor budgets.
Many donors, including USAID, are considering policies to reduce aid allocations to countries and strategically transition select countries away from traditional grant-based assistance. Middle-income countries, in particular, are thought to have increasing fiscal space for public spending and could take on all, or most, of what donor assistance is currently funding, if there is sufficient political will. However, assessing the ability of countries to do so and successfully managing such transitions are challenging.
First, country-level estimates of domestic government spending on family planning, which are critical to assess readiness for transitions as well as to ensure that family planning investments continue, are hard to define.[24] While there are indications that domestic government spending on family planning is growing in a few middle-income countries—signaling that family planning is a domestic priority in some countries—the amounts are not significant in relation to anticipated needs.[25] According to initial estimates from the UNFPA-NIDI Resource Flows Project, for 69 FP2020 countries—comprising low-income countries and some lower-middle-income countries—national government spending accounts for about 30 percent of family planning expenditures, international donors contribute 50 percent, and consumers’ out of pocket spending makes up the remaining 20 percent.[26] Moreover, domestic spending priorities are also affected by health sector and budget structural reforms; many countries are decentralizing functions and budget planning to subnational entities and/or developing universal health care (UHC) schemes, which may or may not include family planning.
Second, each donor also takes a varying approach to country transitions, using different criteria and processes. These processes often do not align across donors and affect the outlook for transition success differently in each country. Family planning assistance is often project-focused, programmed off-budget, and channeled through nongovernmental entities. These approaches reflect the primary donors’ broad structural features, and the historic approach has important implications for the design and eventual success of any country transition.
As the USG looks to transition partner countries away from traditional aid it will be important to:
- Continue to maximize coordination among donors and other partners at a global level to minimize the possibility of a country experiencing an abrupt change in support and a major financing gap;
- Develop a “continuum” approach that recognizes where countries are in terms of their development trajectory and unmet need, and integrates each country’s unique vulnerabilities into assessments; and
- Learn from past transitions by USAID, many lessons of which come from USAID family planning programs, and by other donors (e.g., more recently, Gavi).
Key Ideas and Proposals
Overarching Discussion Goal: Focus on transparent and step-by-step transitions, with the goal of sustainable success rather than reacting in haste to (what we hope will be) short-term funding challenges, especially in terms of USG support.
Participants identified a number of ways to work towards this overarching goal, including:
-
ENHANCE TRANSPARENCY AS A STRATEGY TO REDUCE UNCERTAINTY AND INCREASE THE LIKELIHOOD OF SUCCESS.
- Participants emphasized building on the Modernizing Foreign Assistance Network (MFAN) recommendations.[27]
-
It is critical to envision what transition success looks like across multiple dimensions such as financing, commodities, social norms, health and non-health outcomes. Some examples to consider:
- Aim to get the closest countries to fully transition from all donor support or transition away from USG support as a first step?
- Maximize health improvements? (e.g., Health Systems Strengthening Approach)
- As a related discussion, also ask: are these dimensions and outcomes the same or different compared to current FP2020 goals?
-
There was emphasis on the need for USAID to share, discuss, and publicize the transition strategy with a wide range of stakeholders—implementing agencies, partner countries, other donors, civil society, etc. However, it is important to acknowledge the following:
- There are still several unknown dimensions of possible transition scenarios. Will transition be specific to family planning programs, health sector-specific, or take on whole of country transitions?
- Each of the scenarios (family planning-specific and health-sector wide) would differ in approach and in turn impact each other.
- There was also discussion on the importance of costing and evaluation as part of thinking through a transition plan. Costing is important for potential alternative funders to understand what they are taking on. Evaluation is important for understanding exactly what results might need to be sustained as part of a transition.
-
REVISIT CRITERIA TO BE USED AT DIFFERENT POINTS ALONG THE TRANSITION CONTINUUM FOR FAMILY PLANNING PROGRAMS.
- Participants expressed the need to identify possible trigger indicators/thresholds beyond what USAID currently considers (total fertility rate and modern contraceptive prevalence rate) [28] to start a conversation about transition.
-
Quantitative criteria suggested include:
- On youth bulge and/or security: share of population < 18 years old, or population density
- On equity: coverage among the poor, geographic equity (urban-rural)
- On quality: discontinuation rates
- On health and outcomes for women and girls: births to < 18-year-old girls, child marriage
- Domestic investments for family planning
- Un/underemployment rate
-
Qualitative criteria suggested include:
- Demonstrated commitment or political will to scale or reach the poor as part of the broader enabling environment
- Social norms/demand for family planning
- Ability of private sector to rapidly expand coverage in middle-income countries
- Readiness to implement or scale programs across both public and private sectors
- Readiness (social and financial) of citizens to take on family planning costs themselves
- Participants also mentioned building-in a plan for post-transition monitoring, with defined indicators, in the initial strategy.
- The comparison to MCC-style threshold criteria might also apply here; that is the possibility of setting appropriate indicators with thresholds for when a country is ready to begin discussion about the transition process.
-
INCREASE DOMESTIC SPENDING ON FAMILY PLANNING, ESPECIALLY IN LOWER-MIDDLE-INCOME COUNTRIES AND/OR TOP TRANSITION CANDIDATES.
-
Among other options, participants stressed that donors should create incentives for increased domestic spending on global health priorities, including family planning, taking an integrated approach.
- While co-financing has been used as a strategy for incentivizing domestic country spending, it is not yet part of the family planning landscape. It is worth noting, however, that many global health funders like Gavi, the Global Fund, and the Global Financing Facility (GFF) do employ co-financing requirements as one part of a transition strategy.
- Innovative financing (e.g., Development Impact Bonds, Cash on Delivery Aid) offers one possibility; doing this as part of broader health reforms in-country is another option.
- Establishing a “hand-off” to the GFF for countries at the top of the S-curve was also mentioned. The proposal would be that USAID funds the GFF to transition family planning, and accountability for family planning becomes on-budget.
-
Participants discussed the need to build an integrated “ask” to governments across global health priorities, which considers the fiscal space that is realistically available. Rather than aspirational, participants felt this approach could be operationalized by, for example, combining with multi-year funding commitments as in PEPFAR’s South Africa Partnership Framework. One hypothesis is that this would result in less competition with other global health priorities and would also open the possibility of synergies with other funding streams.
- The “ask” should include a strong and well-integrated investment case, going beyond health to include development more broadly, and targeted to budget-holders in national and subnational governments. While this is being done in some contexts, efforts are somewhat ad-hoc and not connected to the budget allocation process.
-
Among other options, participants stressed that donors should create incentives for increased domestic spending on global health priorities, including family planning, taking an integrated approach.
-
TAKE A “TOTAL MARKET APPROACH” TO TRANSITION.
- As USG support is reduced, plan for sustaining and/or increasing provision by private, not-for-profit, and NGO partners, including faith-based providers, that help ensure access to high-quality voluntary family planning programs. Drawing on experiences in Latin America was suggested.[29]
- Relatedly, building capacity for governments to contract with such providers (note: also discussed with PEPFAR in the context of partnership frameworks); this may include building capacity of payers/purchasers as one part of broader health reforms.
-
TO REINFORCE AND BUILD UPON LESSONS FROM PREVIOUS EXPERIENCES, SET UP A PROJECT, INITIATIVE, OR CLEARINGHOUSE ON TRANSITION (OR BUILD THIS INTO FP2020).
- USAID has a strong track record of successfully transitioning family planning programs in some 15 countries by planning and preparing for long-term sustainability.
- Collating, publishing, and discussing lessons learned from past family planning transitions, including USAID transitions more broadly, as well as past PEPFAR partnership frameworks, could serve as a helpful repository. One option would be to dedicate a section of the USAID-funded Knowledge for Health (K4H) to transition.[30]
-
RECONSIDER AND STRENGTHEN BROADER APPROACHES AND STRATEGIES TO TRANSITION.
- Another issue raised includes working on building capacity to shift cultural and social norms related to the adoption of family planning—this includes working with traditional leaders, faith-based leaders, and others.
- The idea of staggered transitions with a focus on continued support for programs for young people and vulnerable, harder-to-reach communities was discussed.
- Identifying transitions that experience backsliding during or after their implementation was raised. Taking an intentional approach to responding to backsliding and having a tool kit that includes a range of potential corrective actions would be helpful.
- Additional suggestions included bringing in “other partners” outside of family planning and extending beyond health circles; using language that resonates outside internal family planning circles (i.e., tailor terminology for ministries of finance vs. ministries of health vs. US policy audiences vs. other countries, etc.).
- Prospectively evaluating and developing scenarios, using portfolio review data, creating dashboards of appropriation-obligation calendars, and informing a broad range of partners was mentioned.
- Use the information collected to hold both donor and partner governments to account, share data and other relevant information with civil society in partner countries and in the US to enhance budget and performance accountability (note: some budget work with civil society organizations is already underway).
- There was mixed feedback on using the term “graduation.”
III. Commodities
Problem Statement and Background
The sustainability of contraceptive commodities provision remains at risk due to uncertainty about future donor support, especially from the US. This is further exacerbated by existing challenges including dependence on donors to fund family planning commodities, a lack of alignment across contraceptive supply chains, and the expected rapid growth in demand due to the youth bulge.
Figure III-A
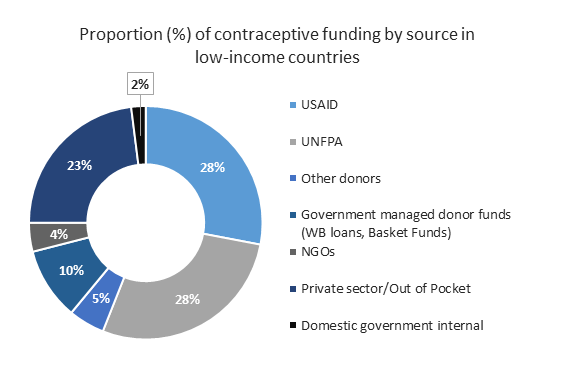
Many countries, especially low-income countries, continue to depend on donors to finance a large share of family planning commodities and related support (e.g., forecasting, procurement, supply chain, and logistics). The Reproductive Health Supplies Coalition (RHSC) reports that within the 69 FP2020 countries, users directly purchase 58 percent of commodities.[31] Slightly less than half (45 percent) are provided through either donor (30 percent) or domestic government (15 percent) financing. The latter represent subsidies that may or may not be targeted to the poor or most vulnerable. In low-income countries, the proportion of commodities provided by donors is much higher, with domestic government funding accounting for a mere 2 percent (see Figure III-A).[32]
While there have been important advancements in strengthening contraceptive procurement and supply chains, existing mechanisms are not aligned across the health sector and, therefore, not necessarily maximizing efficiencies. In many LMICs, there are still parallel supply chains for family planning commodities—and other global health commodities, more broadly. Moreover, reliance on two major central contraceptive procurers (USAID and UNFPA) introduces both benefits and some risks for the sustainability of family planning commodity supplies. In addition to possible reductions in US funding, UNFPA Supplies, which provides about a quarter of all contraceptive commoditites in FP2020 countries, is facing a significant funding shortfall. These uncertainties create the impetus to address gaps and harmonize approaches across donors and other key actors.
Despite significant progress in increasing the number of women and girls worldwide using modern contraception in line with the FP2020 goal, analyses suggest there are still significant numbers of women and men who want to avoid pregnancy but are not using a modern method. Moreover, the number of women who rely on modern contraception in LMICs is projected to grow. Projections based on varying growth trajectories suggest there could be between 490 and 550 million contraceptive users by 2020 in 135 LMICs—this would result in an estimated 37 to 97 million additional users compared to 2016 levels.[33] And, most of this need will be concentrated in some of the lowest-income countries, which also have the fewest resources available.
Uncertainty about future donor support introduces substantial risks to meeting the contraceptive needs of the growing number of women and men entering their reproductive years, especially given donor dependence in high-need lower-income countries. Furthermore, if financing from donors and domestic governments remains flat—or decreases—the cost burden could shift to users who already contribute the largest share to family planning commodity purchases. Recognizing there is no silver bullet, a set of reinforcing and catalytic approaches that take into account USG uncertainties are needed to meet anticipated increases in demand for family planning in the short-, medium-, and longer-term.
Key Ideas and Proposals
Overarching Discussion Goal: Advance toward satisfying the demand for family planning commodities, while also increasing sustainability and planning for uncertainty in future donor support.[34]
Participants identified opportunities to decrease vulnerabilities and increase resilience across donors, domestic governments, and the private sector (both not-for-profit and for-profit), including:
-
WHILE CHALLENGES AROUND PROCUREMENT AND DISTRIBUTION OF FAMILY PLANNING COMMODITIES ARE RELEVANT TO OTHER GLOBAL HEALTH AREAS MORE BROADLY, SOME COMPLEXITIES ARE UNIQUE TO FAMILY PLANNING.
- Most—though not all—health commodities are provided as one product for a specific purpose, e.g., a vaccine for disease prevention or a specific curative drug. In contrast, participants acknowledged that family planning programs seek to maximize the number of products available (contraceptive method mix) to meet the wide range of needs across diverse populations. Furthermore, short-term methods (e.g., pills, condoms, and injectables) require continuous, uninterrupted product resupply to clients.
-
While the issue of fragmented and parallel supply chains applies to the global health commodity landscape more broadly, participants discussed complexities specific to family planning.
- For example, current capacity to support global family planning procurement for the public sector is housed within two major organizations—USAID and UNFPA. Both actors, therefore, are central to the planning and designing of strategies to manage possible “shocks.”
- USAID relies on US FDA-approval (or in some cases, approval by a Stringent Regulatory Authority or WHO prequalification) as the basis for procurement, while UNFPA uses WHO prequalification and country-level approvals for contraceptive procurement.
- Managing multiple products and multiple manufacturers for the same/comparable products (e.g., implants), which may have different lifespans and specialized procedures for insertion/removal, creates added complexities.
- One overarching point was that the quality of family planning commodities is important and needs to be integrated into all proposed approaches.
-
ENHANCE COLLABORATION AROUND STRATEGIC RESOURCE ALLOCATION FOR FAMILY PLANNING COMMODITIES, OVER THE SHORT-, MEDIUM-, AND LONG-TERM.
-
In the short-term, participants stressed the need to enhance efficiencies at the global level by increasing data sharing and synchronizing strategic planning among the leadership of existing global platforms, including the FP2020 Reference Group, the RHSC Executive Committee, the GFF Donor Committee, as well as others outside the family planning space.
-
One suggested idea was to commission short- to medium-term contingency plans to prioritize donor resources available for family planning commodities from existing sources, as well as newly available funding streams, such as SheDecides.
- It will be important to coordinate outreach and fundraising efforts to cover immediate and anticipated mid-term gaps.
- This approach should also recognize that coordination is most effective when there is direct engagement by decision-making entities (e.g., governments, providers from the private and faith-based sectors, donors, etc.) to link decisions with financial flows.
-
One suggested idea was to commission short- to medium-term contingency plans to prioritize donor resources available for family planning commodities from existing sources, as well as newly available funding streams, such as SheDecides.
-
Another proposal was to improve understanding of GFF’s current, and potential future, intersections with family planning commodity provision.
- While GFF does not currently procure family planning commodities, closer engagement would be valuable to understand the role that GFF might play vis-à-vis family planning commodity procurement, as well as supply chain strengthening and harmonization across the health sector, more broadly.
- Over the medium-term, participants suggested increasing the transparency of global, country, and local procurement to minimize overpayment, mark-ups, and large price variations, as well as resource misallocation.
- In the longer-term, resources will be needed to develop new contraceptives, and to introduce new and newly adapted methods with an eye toward growing the method mix.
-
In the short-term, participants stressed the need to enhance efficiencies at the global level by increasing data sharing and synchronizing strategic planning among the leadership of existing global platforms, including the FP2020 Reference Group, the RHSC Executive Committee, the GFF Donor Committee, as well as others outside the family planning space.
-
IDENTIFY OPPORTUNITIES FOR GLOBAL ACTORS TO FURTHER HARMONIZE STRUCTURES AND PLANNING AT THE COUNTRY LEVEL FOR FAMILY PLANNING COMMODITIES—AND EXPLORE OPPORTUNITIES FOR SYNERGIES WITH OTHER HEALTH COMMODITIES.
- Overall, the importance of focusing on structural factors was mentioned. Among the ideas discussed were ensuring provision of family planning commodities is included as part of broader health reforms in-country; continuing and accelerating supply chain integration where possible; and supporting, in tandem, larger health commodity supply chain efficiency, effectiveness, and sustainability.
-
Short-term ideas included:
- Expanding upon and harmonizing the Country Investment Plan and GFF’s Investment Case as they relate to family planning commodities;
- Recognizing the role of decentralized decision-making at the country level, formally documenting its impacts on commodity forecasting, procurement, and supply chain systems; and
- Defining key indicators that demonstrate when countries have matured both in terms of social norms and private sector capacity, with an eye toward increasing private sector service delivery as a share of contraceptive commodity provision (e.g., Indonesia is one example of a mature middle-income country).
-
Medium-term ideas included:
- Strengthening private sector procurement in select settings, possibly by expanding implementation of successful models of pooled procurement designed to support the private sector (both not-for-profit and for-profit). Examples include MedSource in Kenya and DoctorStore in India (which includes online shopping), available to individual providers.
- Prioritizing donor and country financial flows to essential components of family planning commodities and supply chains. This includes supply chain management information systems (MIS), data collection, and analysis, which should be considered an important public good.
- Ensuring adequate support to the human capacity needed to manage existing/new IT approaches and to analyze data for quality, and accurate analyses to support critical decision-making.
-
Over the longer-term, participants mentioned continuing efforts to simplify and harmonize regulatory approval to improve product access, especially across sub-Saharan Africa, and to facilitate product movement across borders to maximize flexibility of global suppliers to fill supply gaps.
- Early lessons from PEPFAR and other organizations in addressing price and regulatory hurdles with ARTs should be reviewed and incorporated, as applicable.
-
SUPPORT ASSESSMENTS TO BETTER UNDERSTAND THE OVERALL COMMODITIES LANDSCAPE AND IDENTIFY POTENTIAL GAPS AND POSSIBLE EFFICIENCIES.
- Participants acknowledged the value of existing RHSC studies at the global level, but also pointed to outstanding questions around defining the entirety of the market and analyzing investments in terms of Couple Years of Protection (CYP) and changing method mixes, which are increasingly maturing to expand provision of long-acting reversible contraceptives (LARCs).
- At the national level, market segmentation within countries will often require better data than are currently available; a more holistic understanding of public, private, faith-based, insurance schemes, etc., is needed.
- Overall, there is a continued gap in understanding who the market is failing and designing effective responses in this space; management information systems are a critical link between service demand and projected need.
-
Continue to build on ongoing analyses of S-curve country status and demographics to predict global method mix demand and inform national and global marketplaces (e.g., Kenya is a leader in this process).
- Linking demographic and S-curve analyses will be important to provide mid-term estimates of global demand for LARCs.
- Increase communication and outreach to experts and policymakers to reinforce the technical and financing leadership role the USG plays as well as the expected increase in demand for family planning in the coming years.
-
ENHANCE PROCUREMENT COORDINATION ACROSS PUBLIC AND PRIVATE SECTORS TO FURTHER IMPROVE PRICING AND ENSURE CONTRACEPTIVE SUPPLY SECURITY AS DEMAND GROWS.
-
In the short-term, it could be beneficial to explore procurement and broader supply chain- related lessons from other global entities and mechanisms including, but not limited to, Gavi and the Global Fund. Some specific suggestions are as follows:
- Coordinate a learning meeting between Gavi, the Global Fund, and family planning procurers to share lessons learned.
- Set the stage for decision-making by defining questions and related indicators to determine if and how to design future global market strategies in family planning to support procurement in the public and private sectors.
-
Commission studies and assessments to understand the potential benefits and costs of pooled procurement mechanisms. It would be important to understand if/how such approaches could help strengthen relationships with contraceptive commodities manufacturers, secure better prices, and ensure supply security in the public and private sectors.
- Draft a set of scenarios for potential pooled procurement approaches to present to FP2020, RHSC, and GFF for consideration.
- Define a study to model a “Gavi-type” approach to provide global market and long-term symbiotic partnership with manufacturers to ensure continuous supplies of commodities.
- Considering the private sector is the primary source of commodities in many middle-income countries, it would also be important to study and better understand possibilities for centralized procurement for the “whole of private sector.”
-
Where feasible, participants discussed the possibility of introducing commodity co-financing for highly dependent partner countries in the medium-term. Some outstanding questions to consider:
- How to do this if not via UNFPA?
- Possible stand-alone platform alongside USAID procurement that allows co-financing or buy-ins to obtain access to prices?
- New procurement public-private partnership that USAID could buy into?
-
When appropriate to the environment, participants also suggested considering other financing mechanisms to support local procurement, such as guarantor processes (insurers)?
- Further, how could this be balanced by local/regional manufacturing capacity as part of economic development and development sustainability?
- For all approaches, discussions focused on matching the best country candidates for testing novel interventions that decrease the need for external financing.
-
In the short-term, it could be beneficial to explore procurement and broader supply chain- related lessons from other global entities and mechanisms including, but not limited to, Gavi and the Global Fund. Some specific suggestions are as follows:
-
EXPLORE THE POSSIBILITY OF A “GLOBAL PLANNING SUMMIT” ON FAMILY PLANNING COMMODITIES.
- As planning for commodities is a medium- to long-term process, there was discussion around the possibility of a global planning summit to help ensure that contraceptive supply grows commensurately with demand. The purpose would be to review the status of global manufacturers and suppliers, and possibly to design medium- to long-term approaches for meeting projected growth in contraceptive demand. In addition to the key public sector procurers, participants suggested coordination with larger entities supporting private sector providers, such as insurers and groups like MedSource in Kenya and DoctorStore in India. By expanding the groups engaged, the global summit could contribute to a global “whole of market” understanding of manufacturing capacity and opportunities to increase efficiencies in procurement and logistics management for family planning commodities.
[1] FP2020, FP2020: The Way Ahead, 2017, Available at: http://progress.familyplanning2020.org/user/data/resources/download/FP2020_ProgressReport_PRINT_Single_LoRes.pdf, see page 6.
[2] For more information, see CGD’s Aligning to 2020 Working Group Report (Silverman R, Glassman A, Aligning to 2020: How the FP2020 Core Partners Can Work Better, Together, Center for Global Development, 2016. Available at: /sites/default/files/Aligning-to-2020.PDF).
[3] For an overview of current efforts to track domestic government expenditures for family planning see Track20’s report (Stover J, Chandler R, Expenditures on Family Planning in FP2020 Focus Countries in 2015, Track20, December 5, 2017. Available at: http://www.track20.org/download/pdf/Expenditures_Assessment_12.5.17.pdf).
[4] Wexler A, Kates J, Lief E, Donor Government Funding for Family Planning in 2016, Kaiser Family Foundation, December 5, 2017. Available at: https://www.kff.org/global-health-policy/report/donor-government-funding-for-family-planning-in-2016/.
[5] Kaiser Family Foundation, President Signs FY18 Omnibus Bill, March 22, 2018. Available at: https://www.kff.org/news-summary/congress-releases-fy18-omnibus/.
[6] Kaiser Family Foundation, White House Releases FY 2019 Budget Request, February 13, 2018. Available at: https://www.kff.org/news-summary/white-house-releases-fy19-budget-request/.
[7] Family Planning Countries, USAID, last updated February 8, 2018. Available at: https://www.usaid.gov/what-we-do/global-health/family-planning/countries.
[8] Kaiser Family Foundation analysis of data from OECD CRS database, accessed January 8, 2018.
[9] Kaiser Family Foundation, UNFPA Funding & Kemp-Kasten: An Explainer, May 12, 2017. Available at: https://www.kff.org/global-health-policy/fact-sheet/unfpa-funding-kemp-kasten-an-explainer/.
[10] Kaiser Family Foundation, The Mexico City Policy: An Explainer, June 1, 2017. Available at: https://www.kff.org/global-health-policy/fact-sheet/mexico-city-policy-explainer/.
[11] Moss K, Kates J, How Many Foreign NGOs Are Subject to the Expanded Mexico City Policy? Kaiser Family Foundation, December 4, 2017. Available at: https://www.kff.org/global-health-policy/issue-brief/how-many-foreign-ngos-are-subject-to-the-expanded-mexico-city-policy/.
[12] For more information, refer to USAID’s Family Planning Program Overview (USAID, Family Planning Program Overview, April 2013. Available at: https://www.usaid.gov/sites/default/files/documents/1864/fp_overview.pdf). In 2003, an initial set of 13 priority countries was selected based on USAID’s allocation formula; 11 countries were added to the priority list under the Obama administration’s Global Health Initiative. More details can be found on page 8 of CGD’s Working Group Report (Silverman R, Glassman A, Aligning to 2020: How the FP2020 Core Partners Can Work Better, Together, Center for Global Development, 2016. Available at: /sites/default/files/Aligning-to-2020.PDF).
[13] See Track20’s one-pager on mCPR growth (Track20, The S-Curve: Putting mCPR Growth in Context, October 2017. Available at: http://www.track20.org/download/pdf/S_Curve_One_Pager.pdf).
[14] A list of FP2020’s focus countries can be found on the FP2020 website (FP2020, All Countries. Available at: http://www.familyplanning2020.org/entities).
[15] Rose S, Collinson E, Kalow J, Working Itself Out of a Job: USAID and Smart Strategic Transitions, Center for Global Development, December 2017. Available at: /sites/default/files/working-itself-out-job-usaid-and-smart-strategic-transitions.pdf.
[16] More information on SheDecides can be found at: https://www.shedecides.com/.
[17] For details on the FP2020 Reference Group, see the FP2020 website (FP2020, The FP2020 Reference Group. Available at: http://www.familyplanning2020.org/about-us/reference-group).
[18] See page 83, Figure 5 of FP2020’s latest progress report (FP2020, FP2020 The Way Ahead, 2017. Available at: http://progress.familyplanning2020.org/user/data/resources/download/FP2020_ProgressReport_PRINT_Single_LoRes.pdf).
[19] For a more detailed description, refer to Track20’s report on family planning expenditures (Stover J, Chandler R, Expenditures on Family Planning in FP2020 Focus Countries in 2015, Track20, December 5, 2017. Available at: http://www.track20.org/download/pdf/Expenditures_Assessment_12.5.17.pdf).
[20] Experience in Latin America shows that progress of family planning programs was sustained following USAID graduation and phase-out, driven by institutionalizing family planning in the public, NGO and private sector. Many governments increased procurement budgets or developed line items, and sustained their commitments over the years. See pages 54-55 in MEASURE Evaluation’s report on Family Planning in Latin American and the Caribbean (Bertrand J, Ward V, Santiso-Galvez R, Family Planning in Latin America and the Caribbean: The Achievements of 50 Years, MEASURE Evaluation, 2015. Available at: https://www.measureevaluation.org/resources/publications/tr-15-101).
[21] More information can be found in a UNICEF press release (UNICEF, New funding will allow countries to secure sustainable vaccine supplies and reach children more quickly, December 13, 2017. Available at: https://www.unicef.org/media/media_102311.html).
[22] More information can be found on PAHO’s Revolving Fund website at: http://www.paho.org/hq/index.php?option=com_content&view=article&id=1864&Itemid=4135.
[23] More information on the International Finance Facility for Immunization can be found at: https://www.iffim.org/.
[24] More details are in the FP2020 progress report (FP2020, “Indicator 12: Domestic Government Expenditures On Family Planning” in FP2020 The Way Ahead, 2017. Available at: http://progress.familyplanning2020.org/en/measurement-section/domestic-government-expenditures-on-family-planning-core-indicator-12).
[25] Commitments from three countries, India, Bangladesh, and Indonesia account for the lion’s share of the $4 billion pledged by lower-middle-income country governments; though it is important to note that some countries have not yet delivered on commitments made at the 2012 Summit. For more information, refer to a CGD blog (Silverman R, Family Planning Summit Raises Much-Needed Funds. Now It’s Time for Donors to Stop Being Polite and Start Getting Real, Center for Global Development Global Health Policy Blog, July 13, 2017. Available at: /blog/family-planning-summit-raises-much-needed-funds-now-its-time-donors-stop-being-polite) and a Devex article (Edwards S, How significant were the pledges at the London Family Planning Summit?, Devex, July 26, 2017. Available at: https://www.devex.com/news/how-significant-were-the-pledges-at-the-london-family-planning-summit-90688).
[26] FP2020, FP2020: The Way Ahead, 2017, Available at: http://progress.familyplanning2020.org/user/data/resources/download/FP2020_ProgressReport_PRINT_Single_LoRes.pdf, see page 83.
[27] For a list of these recommendations, refer to MFAN’s two-pager (MFAN, Principles for Strategic Transitions from Development Aid, November 2017. Available at: http://modernizeaid.net/wp-content/uploads/2017/11/MFAN-Principles-for-Strategic-Transitions.pdf).
[28] Per USAID’s current strategy to transition family planning programs, as outlined in a 2006 technical note, the trigger indicators used to start the process are total fertility rate less than or equal to 3.4 and modern contraceptive prevalence rate 48 percent or greater. USAID’s Office of Population and Reproductive Health is currently revising its strategy. In addition, USAID is also developing agency-wide transition metrics.
[29] Examples of countries in the LAC region that have successfully graduated from USAID Family Planning assistance include Brazil, Chile, Colombia, Mexico, Jamaica, El Salvador, Nicaragua, Honduras, Peru, Paraguay, and the Dominican Republic. Refer also to MEASURE Evaluation’s 2015 report (Bertrand J, Ward V, Santiso-Galvez, Family Planning in Latin America and the Caribbean: The Achievements of 50 Years, MEASURE Evaluation, 2015. Available at: https://www.measureevaluation.org/resources/publications/tr-15-101).
[30] More information on K4H is at: https://www.k4health.org/.
[31] Reproductive Health Supplies Coalition, Global Contraceptive Commodity Gap Analysis, 2017. Available at: https://www.rhsupplies.org/uploads/tx_rhscpublications/Global_Contraceptive_Commodity_Gap_Analysis_2016.pdf.
[32] Estimate compiled by USAID, based on Avenir Health data and Global Contraceptive Commodity Gap Analysis Reproductive Health Supplies Coalition, 2016. For more information, refer to the CGD blog on family planning funding (Silverman R, Global Family Planning Funding – What Should Funders Be Thinking About Now?, Center for Global Development Global Health Policy Blog, December 20, 2016. Available at: /blog/global-family-planning-funding-what-should-funders-be-thinking-about-now).
[33] Reproductive Health Supplies Coalition, Global Contraceptive Commodity Gap Analysis, 2017. Available at: https://www.rhsupplies.org/uploads/tx_rhscpublications/Global_Contraceptive_Commodity_Gap_Analysis_2016.pdf, see page 5.
[34] In line with FP2020 indicator 4: “Percentage of women whose demand is satisfied with a modern method of contraception.”
Rights & Permissions
You may use and disseminate CGD’s publications under these conditions.