Recommended
This is a joint post with Rachel Silverman.
In her classic 2011 anthem, Beyonce posited that it was girls “who run the world.” Yet in the world of global health, we worry that Beyonce may be mistaken – from our observations, it appears that women remain severely underrepresented in top leadership positions.
It may seem counterintuitive that the world’s top advocates for women’s health and equity would be missing women leaders within their own ranks. Women’s welfare is perhaps more prominent than ever before in global health circles, as partially evidenced by this week’s massive Women Deliver conference and the Lancet’s corresponding thematic issue on gender. But gender equality issues have been our mind lately, with the new book published by Sheryl Sandberg (a member of the CGD’s Board of Directors) on women in work and leadership and Anne-Marie Slaughter’s article on women’s roles last year. And Foreign Policy published a list of “the 500 most powerful people on the planet” of which a measly ten percent were female, along with another piece noting how few think tanks are run by women. From our own experience within the global health ecosystem, it’s hard not to notice the relative paucity of women at the top ranks of academia and global health institutions, despite obvious female majorities in global health student bodies and among junior researchers.
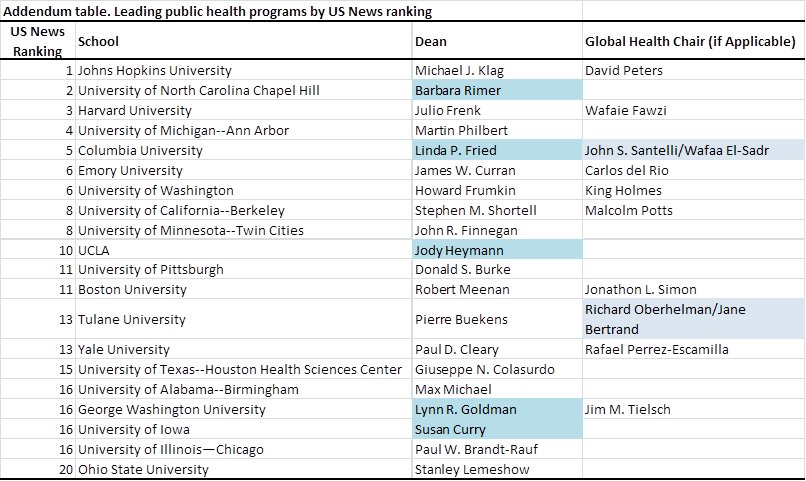
Many global health funding agencies (namely, the Global Fund, GAVI, UNITAID, PEPFAR, PMI, the World Bank, and UNAIDS) have never in their histories had a top-executive who is female. (Granted, UNICEF, UNFPA, PAHO, and WHO are exceptions and are also older institutions.) Given the important role of academia in shaping global health, it’s also notable that only five of the top 20 schools of public health in America (per the US News Ranking) are led by female deans, and that the vast majority of their global health departments are chaired by male professors (see addendum table). Deanships and chairs aside, as one looks at the names in top-ranked faculty lists, it is clear that even tenure-track faculty within global health departments are largely men (see here and here for example).
And what’s remarkable – and well known at least to public health students and professionals – is that despite the differential in sex ratios in global health leadership, the student body in many public health graduate programs and mid-level staff in most policy/advocacy groups have a large female majority. At Harvard and Johns Hopkins, for example, female students account for 71% and 67%, respectively.
It may be that this imbalance needs time; that if we simply wait then today’s female students and junior staff will naturally evolve into tomorrow’s tenured faculty, deans, and global health leaders. But exactly how long before such a transition will occur? Given current trends at the bottom, we might expect such a “demographic transition” towards gender equity to happen quite quickly – say 5 to 8 years – unless there are other factors besides time hindering the gender balance. Notably, in several global health departments, non-tenure track research scientists and associates appear to be majority female, while tenured faculty skew male. It could be that hiring and promotion within tenure-track positions is biased against women, either explicitly or implicitly (i.e. women are pursuing tenure at the same time they are starting families), or that it is a legacy phenomenon from male-dominated times of old, one that will abate as the older cohort gradually retires.
But rather than wait passively for this desired “cohort effect” to gradually improve gender balance, the world of global health should take this issue head-on to determine what the root causes are behind this imbalance, and what needs to be changed within each individual institution.
As a start, global health agencies along with universities, departments of global health, and associated consortia should consider commissioning a report to rigorously examine whether gender imbalances are occurring – what percentage of staff at different levels are female and how many women are there are in top leadership positions? If imbalances are observed – and particularly if the gender balance of leadership does not match the composition of more junior staff or student bodies – institutions would be well served to investigate the factors underlying those disparities and take practical steps to address it. Not simply as a token effort, but because we genuinely believe it to be a problem when the viewpoints of educators and leaders lean heavily towards one gender, particularly when so much of global health focuses on the wellbeing of women and girls. These institutions could take a page from MIT, a school focused on science and engineering, which pioneered a breakthrough study on gender inequality in 1999; more than a decade later, significant progress was reported.
While women may never “run” the global health world (and nor should they, as men offer equally important and valuable voices), equitable and balanced global health leadership is itself a noble goal – one that is feasible within our lifetimes if key institutions demonstrate thoughtful and genuine leadership in this space.
The authors thank different administrators at various schools of public health for advance comments on a previous version of this piece. Victoria Fan (@fanvictoria) is a research fellow and Rachel Silverman (@rasiiii) is a research assistant at the Center for Global Development.
Disclaimer
CGD blog posts reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions.



