Recommended



Healthcare budgets today are under growing pressures, exacerbated by the COVID-19 pandemic and the military conflict in Ukraine, and subsequent energy crisis. In these circumstances, it is more important than ever that governments institutionalise evidence-informed priority setting (EIPS) to transparently allocate finite health resources based on evidence to maximise health benefit and support universal health coverage (UHC).
Improving national EIPS can achieve significant return on investment (ROI). For example, in Thailand, EIPS delivered an estimated 8:1 ROI, and in a brief released today, we estimate a similar 9:1 ROI in India. However, institutionalising priority setting in health is complicated, and there is currently no agreed way to understand and measure progress, plan improvements, or enable cross-country comparison. Current approaches including the WHO Health Financing Progress Matrix (HFPM), and the Joint Learning Network Measuring Health System Efficiency in Low- and Middle-Income Countries, have a wider scope, don’t fully assess the linkage between evidence and decisions, inadequately incorporate the concept of opportunity cost, don’t differentiate among different health technologies, and often rely on subjective judgement rather than factual, detailed documentary evidence.
Today, we release a policy paper, a how-to guide, and data collection tool detailing the iDSI Progression Scale for EIPS (iProSE), with a pilot study in India. Our aim is to give countries, particularly low- and middle-income countries (LMICs), a tool to understand where they are on their EIPS institutionalisation journey so they can plan improvements and track progress. The iProSE scale will also help development partners strategically target support to countries depending on their level of institutionalisation and enable comparisons of different countries’ EIPS progress for policy learning.
Our pilot study showed that India has made remarkable progress from 2016-2022, strengthening its decision-making around what services to purchase, and what price to pay for health technologies.
Aims of iProSE
iProSE is a self-assessment scale that helps countries map and score the extent to which they use evidence to inform their priority setting and resource allocation decisions. It tracks progress on the implementation of key “enabling factors,” such as structures for generating evidence, and then assesses the use of evidence to inform two key sets of resource allocation decisions: what services to reimburse, and at what price to procure health technologies.
iProSE is designed to enable independent self-assessment without external involvement. It uses documentary evidence to minimise extensive stakeholder consultations, making it useful in lower-resource settings. It uses observable milestones of EIPS institutionalisation that are common to most countries, which facilitates cross-country comparison of institutionalisation processes. iProSE can be completed prospectively at regular intervals to show cumulative progress and identify persistent gaps to inform support plans in real time. Or it can be implemented retrospectively to showcase the evolution of policy commitment and identify blind spots.
How the iProSE scale works
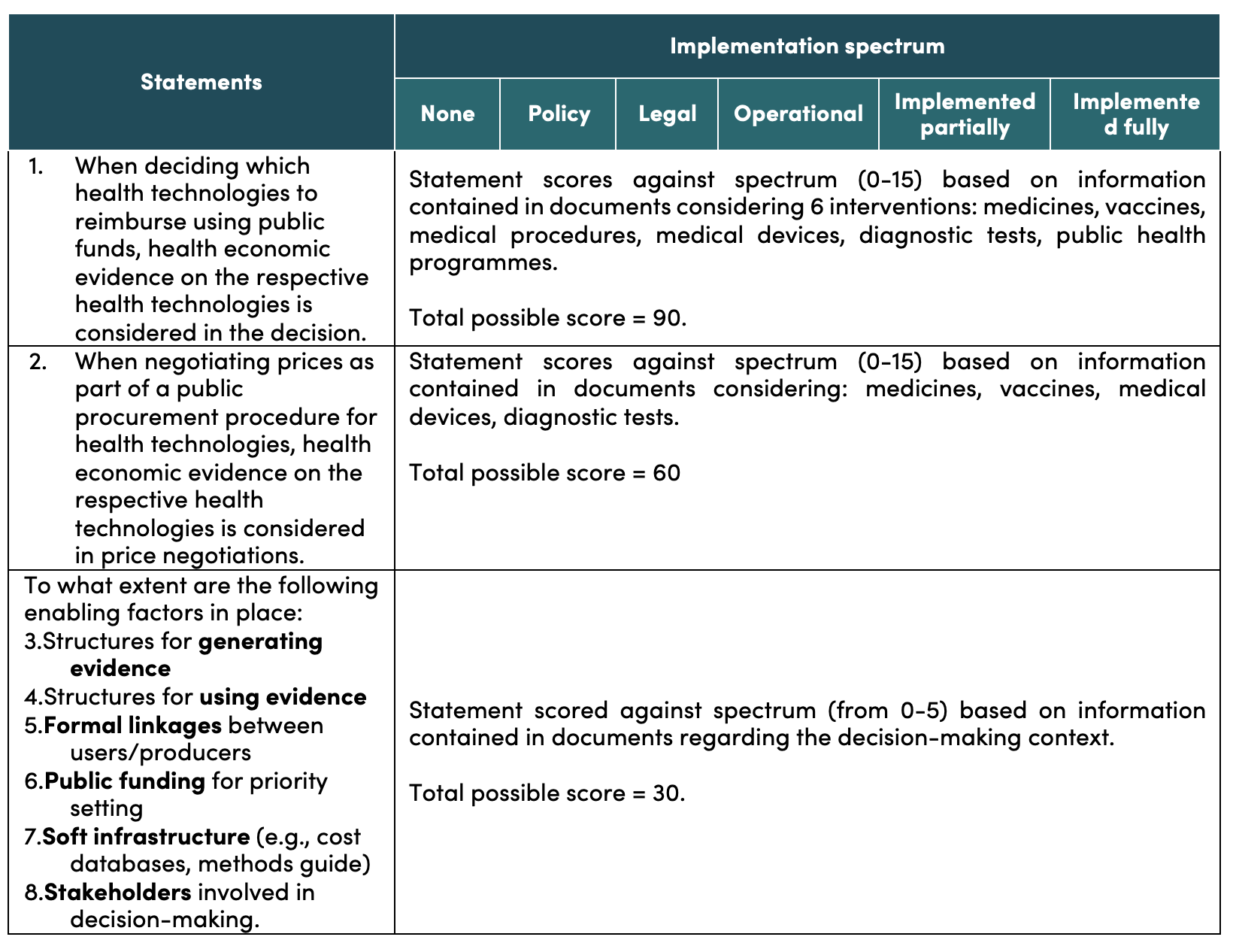
Countries score themselves against eight aspirational statements on EIPS (see table below). Two statements concern decisions on reimbursement and procurement, and six concern enabling factors for EIPS. Countries score statements based on information available in official documents against the implementation spectrum. Upon completion, the tool provides a graphical representation of a country’s score against enabling factors, reimbursement decisions and procurement decisions (disaggregated by health technology), highlighting areas for improvement.
Table 1. Scoring framework
Results from pilot testing iProSE in India
We piloted the iProSE scale in India. We compared India’s position in 2022 and, retrospectively its position in 2016—before the establishment of the Indian Health Technology Assessment agency—to best understand the evolution of EIPS.
We found that India made considerable progress in all areas of the scale from 2016 to 2022.
-
The implementation of enabling factors score increased from 6/30 to 27/30. In 2016, India had a policy intention to embed all six enabling factors for priority setting, but there was no legal mandate, operational process, or implementation. By 2022, all enabling factors are present to a strong degree, with further improvement in the future possible by moving from partial to full implementation of all factors.
-
The procurement decisions score increased from 0/45 to 20/45*. In 2016 there was no evidence that procurement decisions were informed by evidence on costs and outcomes. By 2022, the pricing policy for PM-JAY (India’s largest public health insurance scheme) was published, and a HTAIn analysis of Safety-Engineered Syringes informed procurement decisions and pricing decisions in several states and for a national program. While the progress on EIPS informing procurement “prices” has been limited, this is likely to change with the recent PM-JAY policy on pricing and value-based care.
-
The reimbursement decisions score increased from 23/75 to 40/75*. In 2016 there were instances of evidence generation supporting policy, but there was no formal, systematic process in place. By 2022, complex economic evidence across all health intervention areas was informing some decisions for Ministry of Health programs, PM-JAY, and state governments. This can be further strengthened and systematized to increase evidence-to-policy translation.
* Vaccines were not assessed as a technology for reimbursement and procurement decisions, reducing the total possible score by 15 points.
Our results demonstrate that the iProSE scale can be easily implemented by one knowledgeable expert over a few days, provided they can access required documents and consult key stakeholders. We believe the country progress demonstrated will help sustain political commitment and motivation for priority setting and help policymakers focus on opportunities for strengthening the use of HTA for reimbursement, procurement, and pricing decisions.
What does the India pilot teach other countries?
We believe iProSE and its accompanying tools (how-to guide and data collection tool) can be useful in assessing, monitoring, and accelerating the institutionalisation of EIPS processes and systems in LMICs. We will seek to refine it further based on ongoing and future applications. We recommend that:
- Interested countries use iProSE for conducting baseline assessment of EIPS institutionalisation as a starting point for policy learning, planning, and action, or as a retrospective assessment to demonstrate progress and strengthen political commitment.
- Countries, global health funders, and the healthcare priority setting community consider incorporating iProSE into their own monitoring and evaluation frameworks.
- Countries document lessons learned from applying iProSE in their own settings, and share these to enable cross-country learning, and further development of the scale.
EIPS within institutions can improve value for money in healthcare. The iProSE scale gives countries an easy-to-use self-assessment tool to track their progress and plan improvements for priority setting so they can get more health for their money.
Disclaimer
CGD blog posts reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions.



